Wishing you and yours a safe and happy Canada Day!


Wishing you and yours a safe and happy Canada Day!
Julie Entwistle, MBA, BHSc (OT), BSc (Health / Gerontology)
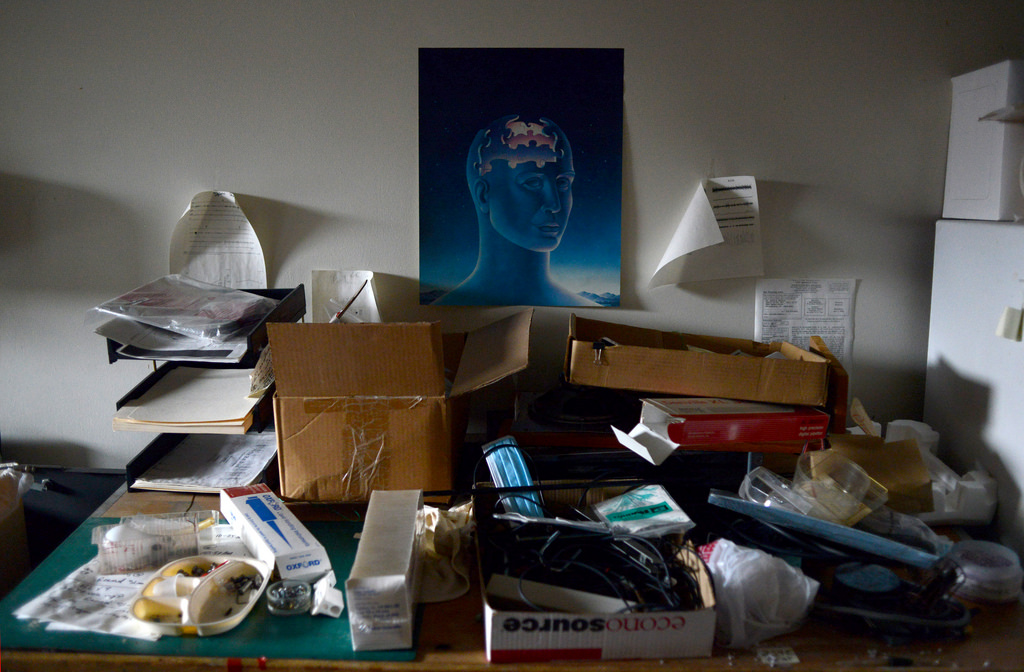
Last stop for Brain Injury Awareness Month – my favorite topic – organization!

Yes, this is my drawer system to store pens, pencils, and markers. And if I find a pencil in the pen drawer look out! Perhaps being organized and knowing how to find what I need when I need it is one of the many ways I manage the demands of being a business owner and mother of four. But the reality is that we all have different levels of energy, tolerance and mental attention and these things can become depleted after a brain injury. So, if you were an energizer bunny with a DD battery before your injury, chances are your new batteries have been replaced with some AAA’s. This means that daily activities will take more time, more energy, and you will need to recharge sooner. So, considering this, do you really want to spend your valuable energy looking for stuff?
Consider that you have 10 units of brain capacity and energy when you wake in the morning. Every activity you have on your “to do” list takes one unit. Going for a walk, preparing supper, managing the laundry, responding to emails, attending an appointment, completing personal care, and having coffee with a friend all drain your battery. Some of these activities are necessary, some can be put off, and others are enjoyable. So what if you spend one unit of energy looking for your phone, keys, that bill that needs to be paid, your agenda, or those new runners you bought yesterday? What activity will come off your list when you have spent your energy to find something that with some organization would have taken you no time at all? Maybe you will call your friend to cancel, or order supper in again. Maybe the laundry will wait to tomorrow, or those emails will just keep accumulating. But this is unnecessary because you had the energy and cognitive ability to manage these things, it just became misdirected.
Often the focus of occupational therapy becomes helping people to organize their activities, their stuff or their time. Schedules and consistency are keys to helping people to understand the size of their battery and the amount of units each activity takes. This can be difficult when working with clients who did not need to be organized before an injury or illness, but the necessity of this following cannot be ignored. Even small steps to help people to be more organized can have a huge impact.
Helping clients with brain injury to become more organized can take many forms, depending on the client, the nature of their problems, and how they previously organized their stuff and their time. What I tend to witness is the time lost and sheer frustration that clients experience looking for cell phones, wallets and keys. Often, cell phones become used as a “second brain” assisting people to maintain a schedule and make appointments (calendar), remember things (task lists), have access to support systems (contacts, calls, text, email), and negotiate their environment (maps and GPS). If this gadget is so important, it is even more important that people know where it is. Having a catch tray by the front door, in their room, or a standard docking station can be helpful. Wallets and keys should also be left in a consistent location. I am sure we can all relate to that feeling of looking for our keys in their usual spot to find they are missing. But if you lack the ability to efficiently look for these, it could completely derail your day.
After the day to day items have a place, then we can work to simplify other spaces that are identified barriers to function. Perhaps the kitchen has become too cluttered to allow for efficient meal preparation, or the bills are piling up because these are lost in a stack of papers. In the world of insurance I find that clients become overwhelmed by paperwork and this results in missed appointments, non-response to time sensitive material, or failure to submit for expense reimbursement. Slowly, over time and with suggestions and tools (filing cabinets, labels, folders, a pen drawer!) clients become able to more efficiently spend their units of energy on things that are more important, or more fun and ideally, learn to transfer these strategies into other life areas independently – like work, school or parenting.
To read more of our articles on brain injury check out our section on Brain Health.

Co-written by Jacquelyn Bonneville, Occupational Therapist and proud member of the LGBTQ community
Have you ever been on vacation to Jamaica, Dominica, or St. Lucia? Have you ever Googled pictures of the beautiful Maldives? Did you know that all of these countries, and some 70 others, have anti-homosexuality laws punishable by fine, imprisonment, or death? Globally we still have a long way to go, but like all progress, we must remain proud of the steps forward we are taking in regards for Lesbian, Gay, Bisexual, Transgender, and Queer (LGBTQ) awareness and rights.
Pride month is celebrated in June in every year in honour of the 1969 Stonewall riots in Manhattan, USA; a turning point for LGBTQ activism. If you don’t identify with this culture you may not feel that pride month is relevant to you, however the spirit of pride month is to embrace diversity and peace, which all of us should celebrate, especially as proud Canadians. This point, and the concept of peace, is even more prominent today considering the recent events in Orlando that resulted in the senseless killing of 49 innocent people as they attended a nightclub frequented by the LGBTQ community.
In honour of pride month, we’d like to offer 3 simple ways you can make your business more LGBTQ friendly:
1. Challenge your assumptions.
It can be easy to assume that everyone is straight; when you ask a man if he has a wife, or a woman if she has a husband, you could be unintentionally making an awkward scenario for a non-straight person. If you have an intake form that only has two gender options (male or female), you could be instantly excluding someone, or causing them to feel uncomfortable about your services.
As therapists we are often in a position of asking about our client’s social supports. Instead of making assumptions, ask more open-ended questions such as “Are you in relationship with someone right now”, “who is your main source of support”, or “do you have a significant other?” Have an “other” option for gender on intake forms, or include sex as well as gender if someone’s sexual organs are relevant to your medical field. Consider expanding “married” on your intake process to include “common law” and “long term relationship”. You’ll still get the information you need, but in a more inclusive way.
2. Don’t be afraid you’ll use the wrong terminology.
My husband’s name is Kelly. Many times people have assumed he would be female: he has been put on the girls’ draw in tennis tournaments, rendered us to win the prize for the “ladies best foursome” in a golf event, and often our mail and solicitation calls are directed to Mrs. Kelly. We’ve all called someone by the wrong name / gender accidentally before. It’s embarrassing – usually they correct us, we apologize, and chances are you’ll never forget their name again. It happens, but in the grand scheme of things it isn’t a big deal.
Gay, lesbian, queer, bisexual, bigender, cisgender, gender fluid, asexual, feminine/masculine of center, intersex, MSM/WSM, pansexual, trans*, two-spirit, ze – what does it all mean? If you are not part of any particular minority group, it can be difficult to know if you’re wording something ‘correctly’ and it may make you uncomfortable. You may even be afraid to offend someone – isn’t ‘queer’ an offensive term? It all comes down to individual preference – and you won’t know until you ask.
Instead of assuming a person is Sir or Ma’am, Mr. or Mrs. based on your assumption of their gender, get used to asking more inclusive, generalized questions as part of your daily routine. There is nothing wrong with asking a client/patient, “What’s your preferred name?” or “How should I address you?” And if you slip and use the wrong pronoun or term in addressing them, simply apologize, correct yourself, and move on. Besides, a good businessperson should have a healthy dose of humility – your clients will respect you more for trying to use their preferred terminology, even if you make a mistake. Don’t worry.
3. Understand some of the systemic barriers LGBTQ persons may face in your system.
Knowledge of some of the challenges in your own business that directly affects persons of various sexual orientations and genders will only make your business more inclusive. Some questions that may be relevant to health care professions include: Can a bisexual person donate blood in your city? Is a transperson legally able to give emergency medical consent if their loved one is unconscious? Will a queer person be safe in a shared hospital room if their partner comes to visit them?
Health care isn’t as easily accessible as you may think. It can be very challenging to find competent medical and rehabilitation practitioners that are educated on health factors more common in certain minority populations, and so not all people feel they can be open with their family doctor or access health care without judgment. Knowledge is power – keep an eye out for changing laws, trends, or factors affecting the LGBTQ population in your area.
In the end, consider adopting some of these strategies into your everyday life, and you’ll be making maximum impact with minimal effort. To quote a Futurama cartoon episode:
“When you do things right, people won’t be sure you’ve done anything at all.”
No one may notice you changed your language, or thank you for making the change – but to that client who needs to know that they’re safe with you, I guarantee you that your choice of inclusive words will make all the difference.
As Occupational Therapists we are lucky to be able to assess our clients holistically, and to consider all of the factors that may be affecting their occupational performance including sexual orientation, gender, sex, and social support networks. We can constantly challenge our assumptions to help develop into even better practitioners.
Happy pride month!

Julie Entwistle, MBA, BHSc (OT), BSc (Health / Gerontology)
Brain injury awareness month continues…this stop: Executive Functioning.
Simply defined, executive functions are the capacities we require to achieve a goal. These are commonly referred to as the “CEO” of the brain because they provide people with the higher order processes that allow us to plan, organize, initiate and complete tasks successfully.
Practically, think about the last time you moved. Moving, as an example, is a simple goal of just wanting to relocate from one place to another. The goal is not the problem: it is the processes and thinking required to manage the transition effectively that can be difficult. Several months before moving you are searching for a suitable place, weighing the pros and cons of each location, checking your budget. Then you make the decision of where to move and you need to deal with your existing location. When do you need to notify your landlord, or when should you list your house? Then, months and weeks before you move there are calls to make to utility companies, mail to redirect, insurance to organize, movers to book and packing to do. What belongings are you moving? What should be sold, donated, discarded? The day of the move is chaotic, stressful, and exhausting. Then for months after you continue to unpack, move things around, find ways to arrange and store your stuff.
Really, your level of executive functioning, or your ability to delegate and enlist support for your areas of weakness, will determine the outcome of your move. So now imagine that you have a brain injury and as a result you feel the same sense of stress, fatigue and frustration with more simple daily tasks, such as planning a meal, sorting your mail, or scheduling your time. This is often how people with brain injury feel on a regular basis.
So, what can occupational therapy do to help? Well, the treatment for executive dysfunction is both broad and simple. It is broad because everyone experiences brain injury differently, and comes into it with varying levels of recoverability. It is simple because it merely involves taking a goal and breaking this down into component parts, manageable chunks, and smaller tasks within the whole.
Returning to the moving example, as an OT, assisting someone who has executive dysfunction with a pending move may involve making checklists with tasks and timeframes, and checking on progress frequently. Personally, I like to take a project approach: calling the goal “Operation Move” and mapping out – start to finish – the metrics for success. Perhaps in month one an “apartment hunting worksheet” is created to help the client summarize all the places they are looking at, the pros / cons, address, and list of questions that need to be answered (price, utilities included, length of lease etc.). Often I encourage my clients to use a smartphone to take photos of the options then we cross reference these and catalogue them to keep things organized. From there, the process continues with checklists for calls to make, addresses to change, ways to organize packing and management of belongings. Ensuring the client is responsible for follow-up via “homework” between sessions and holding them accountable for completion of this aids to developing independence. Really, the therapeutic goal is far more than just ensuring the client is able to move successfully. Rather, it is demonstrating a model and method that can be used for any future transitions, goals or tasks. This ensures success that is transferrable to other events at later dates.
Often, the above strategies are also helpful for people with other forms of cognitive impairment – not just ABI, but could include stroke, dementia, or degenerative neurological conditions that impact how the brain organizes, processes and works through daily tasks. Ask an OT – we know stuff!

Concussions are serious and it is vital that anyone who has suffered this type of brain injury seek help to ensure proper recovery. An Occupational Therapist can help!
Learn more about how to manage a concussion and post-concussion syndrome (PCS) in the following from our OT-V video series:
+
Check out more from our informative Occupational Therapy Video series, OT-V.

Julie Entwistle, MBA, BHSc (OT), BSc (Health / Gerontology)
We cannot (or should not) discuss brain injury awareness without spending time recognizing the family and friends that take on the caregiving role after someone they love has an injury of this nature. Two years ago I co-facilitated a workshop for caregivers of brain injury survivors. What a great event! Not only was this well attended, but the speakers provided an amazing amount of education, skills and insight into how to both cope, manage, and achieve success as the care provider of someone with a brain injury. I wanted to take a moment to highlight my personal takeaways from this event:
Everyone has a story. As someone who lost a brother-in-law to the effects of a catastrophic brain injury, I understand how telling our story – be it about loss, change, remorse, guilt, fear, or triumph can bring people together and has immense therapeutic benefit. Caregivers benefit from collaborating, talking, sharing, laughing, crying and growing together. Our health system needs to create these opportunities, or caregivers need to find ways to make this happen.
Grieve. In my undergrad I studied grief and loss and even worked in hospice. What I realized at our workshop, however, is that the permanence of death allows people to grieve their loss, achieve acceptance, and eventually move on. When dealing with survival from a traumatic event, however, grief is not always experienced as our loved one is still present, albeit different. Yet, our speakers emphasized the importance of grieving: the life that once was, the life that may never be, and the changes and adjustments that have occurred. Caregivers need to let this grief process happen, or should seek support from a trained professional to experience this important emotion.
Find a new normal. Clients, caregivers, and health care professionals need to always consider that the old “normal” may never return. In that case, we all need to collaboratively look ahead to creating a “new normal”. Different does not always have to be bad, and it requires an open and optimistic mind to think that way. For OT’s that means taking the abilities of the individual, considering their resources, and helping them to create that new life of function, fulfillment, meaning and productivity.
Put on your own oxygen mask first. We spoke extensively about the importance of caregivers taking the time to attend to their own personal needs, to have positive coping mechanisms and sources of support. Then, at break I was speaking with a man whose wife suffered a brain injury. He talked about the “airplane analogy” and how this applies to caregivers – put on your own mask before helping another. I smiled and told him that I wrote a blog on that exact topic, with that exact title last year. As he found that analogy practical and helpful, I thought I would share the contents of that previous blog here, to highlight this important third point:
If you have ever travelled by air you are familiar with the drill. Instructions on how to buckle and unbuckle your seatbelt, where the life vest is located, emergency exits, and “should cabin pressure change, an oxygen mask will fall from the overhead compartment…passengers should always put on his or her own mask before assisting children, or a disabled passenger”.
I read a mommy blog the other day that called this the “airplane example” and the writer related this to how moms should approach motherhood. Ultimately the message is this: as a mom, put your own health first because you are useless to your kids and spouse if you ignore your own needs. Really, you can’t help a child with an emergency escape from a crashing plane if you pass out helping them with their mask.
While I do agree that mothers (and fathers for that matter) need to consider their own needs in providing for the family, this is also true of people that provide care to a disabled person. My experience is that often caregivers do not really “elect” that role. They are not trained to be a caregiver, and really just try to do their best with the skills and resources they possess. However, where many fall short is maintaining their own health and wellbeing in dedicating their physical and emotional time to another person: a person with challenging and multiple needs. The job of a caregiver is often 24 hours, and resources don’t often permit, nor does the government provide, sufficient relief from this responsibility. Caregivers are often sleep deprived, suffer from muscle and joint pain in fulfilling their role, and can become isolated and depressed due to the changes they have made to take on these new responsibilities. Sound familiar? This very closely mimics motherhood (especially for new moms).
The answer? Put on your own oxygen mask first. What can you do to breathe easier? What helps you to feel clear-headed, energetic and optimistic? What gives you that ability to stay positive, appreciate and take on your responsibilities with some enthusiasm? The answers are often different for all of us. In the end, figuring out how to wear your oxygen mask first requires you to be honest about your abilities and skills, to utilize the resources available, and to ultimately ask for help if this is needed.
And for us health care professionals? We need to be very careful of the responsibilities we place on caregivers. This is especially true in the medical community where we repeatedly discharge people into the care of family, without family really knowing what the responsibilities will entail. As health care providers our responsibility is always to the client, yet we need to take that extra time to check in with the caregiver, talk about how they are coping and managing and if needed, offer them an oxygen mask.
I hope the caregivers that attended our workshop felt that by spending a day focusing on themselves, expanding their knowledge, and learning the keys to success, that this was one step towards them being able to put their own mask on first. This was highlighted at the end of the day when the caregiver of a survivor, whose loved one was injured 13 years ago gave this advice: “If I could do it again, my priorities would be self, family, then my loved one with a brain injury”. What a great lesson for me to take forward in my practice.
For more posts related to brain injury please visit our Brain Health Archive.
Julie Entwistle, MBA, BHSc (OT), BSc (Health / Gerontology)
“An ounce of prevention is worth a pound of cure.” Benjamin Franklin
In recognition of Brain Injury Awareness month, I thought it would be fitting to start at the very beginning. PREVENTION. Really, it is the best medicine. For now, let’s forget about the symptoms of brain injury and its’ impact on work, home, school, and quality of life. Let’s not talk about how it is assessed and treated. Instead, let’s focus on trying to stop it from happening in the first place.
But even before that, we need to know what we are dealing with. It is well known that brain Injury is the leading cause of death and disability worldwide. In Canada, Traumatic Brain Injury (TBI) is more common than breast cancer, spinal cord injury, HIV/AIDS, and multiple sclerosis (MS) combined. There are approximately 18,000 TBI hospitalizations annually. In the province of Ontario, 25% of the two million people diagnosed with a neurological condition have suffered from a TBI. In 2000-2001 brain injuries accounted for $151.7-million in direct costs to Canadians (1).
By way of distribution, TBI is most common in children (0-19) at 30%, followed by seniors (60+) at 29%. In kids, falls are the most common cause followed by motor vehicle accidents and then sports. In adults, motor vehicle accidents cause the most TBI’s, and in seniors the causes include falls (76%) followed by car accidents (2).
Knowing the causes helps to look at how we can engage in preventative strategies. As an occupational therapist with a background in health promotion, a parent of four, and athlete, here are my thoughts:
Falls
Kids fall all the time, so how can we prevent that? Well, there is a difference between a child falling when walking, running or jumping, versus falling from, say, a shopping cart, off of a playground structure, or from a tree they tried to climb. Falls from bikes, skateboards and scooters are going to happen – and a helmet can mean the difference between a head injury and not. The bottom line is that falls in kids are best prevented by proper adult supervision. Yes, it is that simple.
In seniors, falls take on a different form. They are not from carefree or reckless behavior, but often happen when someone is just trying to go about their day by having a shower, coming down the stairs, or taking a leisurely walk. Seniors need to be attuned to the physical, balance and vision changes they are experiencing as they age, and need to consider the importance of anti-slip mats in the bathroom, removing scatter mats, installing grab bars or railings, and the benefits of a walking stick or cane when outdoors. Seniors need to engage in regular exercise and activity to maintain bone density, mobility and intact balance. They have to be very careful when living with pets or when trying to negotiate places that are cluttered or dark. Awareness of declining abilities is the first key to addressing these properly such that a prevention plan can be developed that will ultimately improve safety and reduce the risks. Note that the services of an occupational therapist can be pivotal in creating this safety plan.
Check out our OT-V episode “Fall Prevention” for more helpful information.
Motor Vehicle Accidents
Like falls, despite our best intentions, these can and do happen. The issue here is trying to minimize the risk and optimize the outcome. Safe drivers are attentive, undistracted, and alert. They travel at safe speeds, approach intersections with caution, stop behind the line, pass when appropriate, and recognize that rushing to get somewhere on time is useless if it means you never get there at all. Safe drivers don’t text or hold a phone to their ear, don’t eat a hamburger and steer with their knees, and don’t drive when tired. If you are one of these drivers you are going to increase your chances of avoiding a collision, and lower your chances of being the cause. Unfortunately, however, not everyone is a safe driver. So, all the rest of us can do is wear our seat belt, buy a car with a good safety rating, make sure everyone in the car is buckled properly, make sure the headrest is at a proper height, put loose belongings in the trunk (I know of a child who got a head injury from a flying jar of pickles that escaped the grocery bag during a collision), and follow the rules for child seats.
Sports
I am an avid athlete and have pretty much played or tried every sport. There are very few sports I dislike and I honestly feel that sports can be the most positive and influential outlet for young people, and one of the most engaging and social outlets for adults. The issue is that sports seem to be becoming more and more competitive, kids and adults are getting bigger and stronger, and the culture of some sports has changed from friendly competition to all-out war. Preventing head injury in sport can include outfitting your kids with proper equipment (many hockey parents spend more on a stick than a helmet), ensuring they are playing at their level, monitoring the coaching influence and team culture to make sure this is appropriate, and my favorite is from the book “The Secrets of Successful Families” and includes that the only job of a parent in organized sport is to “shut up and cheer”. No parent should be on the sidelines encouraging reckless, mean or harmful behavior. The results can be devastating. And if you are concerned about your child’s risk of head injury in sport, know that there are many other sports that reduce the risk but are equally as challenging, competitive, fun and have the same physical, cognitive and developmental benefits.
So, let’s start our recognition of Brain Injury Awareness Month by practicing prevention. It does not have to be easier said than done.

Julie Entwistle, MBA, BHSc (OT), BSc (Health / Gerontology)
As a newer vegetarian, and someone who spends most days on the road, I am always looking for quick, but decent, lunch options. While in an ideal world I would prepare my lunches and snacks ahead of time (including hand sanitizer!), sometimes life takes over and I am rushing out the door unprepared. On some days that may result in me being undernourished and not eating again until dinner, on other days it does have me searching for healthy stuff en route. So here is my list of the healthiest but fast meal options that are under 300 calories but can be grabbed quickly, as listed by restaurant name:
SUBWAY
Veggie Delight (whole wheat bread without cheese or mayonnaise) 230 Calories
MCDONALDS
Side Garden Salad (no dressing) 40 calories
Chipotle Chicken Snack Wrap® with Grilled Chicken 230 calories
Grilled Chicken Snack Wrap® 230 calories
WENDY’S
Full Asian Cashew Chicken Salad (no dressing) 190 calories
Chicken Go Wrap Grilled 260 calories
PITA PIT
Garden Pita (no cheese or condiments, whole wheat pita) 227 calories
Tuna Pita (no cheese or condiments, whole wheat pita) 285 calories
Turkey Breast (no cheese or condiments, whole wheat pita) 286 calories
STARBUCKS
Perfect Oatmeal (plain) 140 calories
Spinach, Roasted Tomato, Feta and Egg White Wrap 280 calories (my personal favorite with the nutrition value quickly wasted by my latte add-on).
TIM HORTONS
Chicken Ranch or Salad Wrap Snacker 190 calories
Chipotle Chicken Wrap Snacker 200 calories
Chili 290 calories
Soups (no bun) 80 – 230 calories
HARVEYS
Warm Grilled Chicken Salad (no dressing) 150 calories
Warm Grilled Chicken BLT Salad (no dressing) 210 calories
Grilled Chicken Sandwich (no cheese or condiments) 280 calories
BURGER KING
Tendergrill Caesar Salad (no dressing) 250 calories
Hamburger (no cheese or condiments) 260 calories
Veggie Burger (no cheese or condiments) 270 calories
QUIZNOS
No under 300 calorie meals.
Of course, calories are not the only consideration when consuming a healthy lunch. However, this measure can provide an easy metric when looking for something fast while trying to avoid the unnecessary calories found in heavy carbs and bad-fat common to fast food meals. For drinks, stick to water as not only is this often free (tap water) with your meal, but it provides an opportunity to rehydrate which is also important.
I hope this list helps you to also pick healthier options when on the road.

Julie Entwistle, MBA, BHSc (OT), BSc (Health / Gerontology)
As an occupational therapist, business owner, and MBA, I can’t help but to reflect on the colossal legislation that is the Accessibility for Ontarians with Disabilities Act, or AODA. If you are not familiar, the AODA is Ontario’s way of making the province accessible by 2025 by addressing the following key areas so that people with disabilities can more fully participate in their communities: customer service, employment, information and communication, transportation, and design of public spaces.
Here are some real examples of poor service that demonstrate why such a legislation is needed:
Would you, or the people of your organization, make these mistakes? Do you even know what the mistakes are? Does your organization know how to manage these situations better, with tact, and preventatively?
My business hat tells me that business owners will respond to the AODA in one of three ways: “it won’t happen to me”, “tick the box” or “this is important”.
It Won’t Happen to Me
These are the group of owners that will ignore the legislation and not fear the result. They won’t care about the impression they leave on people that may try to access their services but can’t. Or the people that may try to get into their building and can’t. Or the people that will try to use their website and can’t. They won’t concern themselves with the comments lost consumers may spread about how they felt or how unfortunate it was to encounter such correctable barriers. These owners feel confident in the fact that not being able to meet the needs of a disabled customer will not impact their reputation or bottom line. They sleep well and don’t concern themselves morally or ethically with the possible ill experience of one lost consumer who really just wanted to have equal access.
Tick the Box
These owners will review the legislation and will make sure they do the bare minimum. They will send someone from HR, or one employee, to a one hour seminar on how to provide service to people with disabilities and that person will return and teach the rest of the team. They will “tick the box” that they did some AODA customer service training and will hope that this is enough. These owners do care about potential customers with disabilities and recognize that while 15% of people in Ontario have a disability, even more are caregivers, parents of a disabled child, or that the demographic shift with the aging population will make AODA even more important. While they care, they don’t care enough to actually ensure they get it right. They feel the bare minimum will be better than nothing, and will hope that their staff at the least don’t upset or hurt someone that may try to access their building, or their services.
This is Important
This is the group of concerned owners that want to hit the nail on the head. They don’t believe in doing the bare minimum because they are interested in providing amazing service to all customers. These owners are forward thinkers that recognize the growing number of disabled consumers, and see how the ripple effect from one person’s great experience can transfer to a story told to many. These owners want to have caring and compassionate staff that are comfortable helping a visually impaired client sign forms, or a client with a hearing impairment to get information over the phone. They embrace everyone that enters their building and know how to offer great service without saying the wrong thing or without the fear of coming across as condescending or ignorant.
I guess what box you fit into will ultimately depend on your:
1. Risk tolerance – can you tolerate a bad reputation, poor social media reviews or comments, or the threat of being sued over failure to comply?
2. Values – do you care about people with disabilities and the experience they get from your organization? Do you value being seen as caring, compassionate, and accommodating?
3. Resources – do you have the time, interest or resources to invest in thorough and proactive solutions? Will you take the time to explore the options and to provide your team with the most practical and useful training?
4. Goals – is one of your goals to provide exceptional service to all? Do you see a customer as a customer, all having equal value and an equal opportunity to not only benefit from your service, but to also benefit your bottom line? If your goal is business success then the AODA is nothing to ignore.
Let me demystify how my examples earlier could have been handled better:
What kind of owner are you?

Julie Entwistle, MBA, BHSc (OT), BSc (Health / Gerontology)
In June 2016 the Statutory Accident Benefits Schedule will change again. I say “again” because in my relatively short sixteen year lifespan working in auto, the industry has gone through some major plastic surgery. It is becoming less and less recognizable as it is nipped and tucked once more, becoming almost unrecognizable as the mandatory product we all purchase to be covered in the event of an accident.
Since the announcement of the upcoming changes, the common reaction is comparable to the story of Henny-Penny and Chicken-Little who create hysteria after an acorn falls on Chicken-Little’s head. In earlier versions of the Chicken-Little story all the paranoid animals get lured and eaten by the fox. Later versions of course have the animals living happily ever after, or finally understanding Newton’s law.
So, is the sky falling in Ontario’s auto insurance? Well, I won’t say things are all unicorns and rainbows. As of June 2016 all Ontario drivers will be paying relatively the same dollars for 50-98% of the coverage. Attendant care and medical rehabilitation monies are being combined, resulting in reductions in coverage totalling $21K for seriously injured people and $1M for those that are deemed catastrophic. On top of that, the industry will revise the criteria for catastrophic status so less people will qualify in the first place. As a consumer, it is infuriating that my premiums are not changing to the $50 / year that this new coverage is worth. As an OT that has clients running out of monies now, this does seem like the sky is falling. Take for example my 16 year old client with C5 tetraplegia. One million dollars in combined coverage will not last long for someone that is young, has a permanent impairment, who requires 24 hour care (and sometimes the care of two people simultaneously), and who will require a fully accessible home and vehicle so that his basic needs can be met. And that does not even speak to the costs for the many therapies, wheelchairs, lifts and other treatments needed, nor the costs to get him education support and engaging in activities that he will find both meaningful and productive.
From a consumer and client perspective I am concerned. While there is an option to “buy up” for decent coverage, most people don’t exercise this under the “it won’t happen to me” facade. However, as a wanna-be optimist, from a professional and business perspective I can still help a lot of people with $65K or $1M in coverage. That is a lot more money available than the $0 my clients with ALS, MS, stroke, or cancer ever receive.
So, Chicken-Little, Henny-Penny and friends overreacted. They panicked. They caused chaos. I, on the other-hand, am choosing to take the adaptive approach. Where are the opportunities? What is still good about the coverage that remains? Where can I still add value and help people? How can I be proactive instead of reactive? What initiatives can I support that are advocating for client and consumer protection? What can I do in my practice to make $65K and $1M last as long as possible? Call me Julie-Fooley, and perhaps I will be eaten by Fox-FSCO, but I still want to believe in happy endings.